Intravenous Conscious Sedation for Routine Lumbar Injections
Point/Counterpoint
Guest Discussants: Neel Mehta, MD, Jennifer Zocca, MD, Naum Shaparin, MD, Max Snyder, MD
Feature Editor: Jaspal R Singh, MD
The most common type of lumbar (low-back) pain originates in the lower back and travels through the buttock and down the leg. This pain is known as lumbosacral radicular pain or sciatica.
Sciatica is most likely to develop around age 40 or 50. Sciatica causes the sensation of pins and needles, a decrease in motor function, or difficulty performing certain movements that reduce one’s activity level and quality of life.
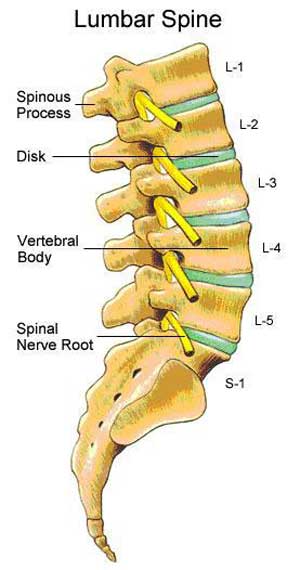
Understanding the anatomy of the spine helps us understand the cause of sciatica. The spinal cord is divided into segments—or levels—according to the nerve roots that branch off. Nerve roots run through the bony spinal canal. In the lumbar and sacrum regions of the spine, a pair of nerve roots exits from the spine at each level.
Spinal stenosis, a narrowing of the disk space, and disk protrusion (also known as a herniated disk) can cause pinching, irritation, and inflammation of the nerve root(s). As a result, people with one or more of these conditions experience low-back pain that can travel to the legs.
To better understand the cause of a patient’s back pain, physicians perform a physical examination and offer diagnostic tests, such as magnetic resonance imaging (MRI) and electromyography (EMG). The information gathered helps doctors determine the extent of the nerve damage and source of the pain, as well as develop a plan for managing pain and other symptoms.
What is a TFESI?
Treatment options for sciatica include lifestyle changes, physical therapy, oral anti-inflammatory or steroid medications, and interventional pain management procedures, such as lumbar epidural steroid injections (ESIs). Read more about ESIs.
A transforaminal ESI (TFESI) is an ESI delivered into the opening at the side of the spine where a nerve root exits the spinal cord, allowing for more concentrated delivery to a specific nerve to directly address the source of pain.
What is conscious sedation?
Conscious sedation—also called moderate sedation or procedural sedation—is a combination of medicines given to help patients relax during a medical procedure by minimizing discomfort and anxiety. It is often used for dental operations, minor surgeries, and other routine medical procedures, such as lumbar ESIs.
The medication is delivered through an intravenous line (in a vein) or an injection into a muscle; it is sometimes given in the form of a pill. When a patient receives conscious sedation medicines, he or she will quickly feel drowsy and relaxed. The patient’s breathing will slow and blood pressure may drop a little.
Under conscious sedation, the patient will be somewhat awake or lightly asleep. He or she will be able to respond to questions, but may not remember any or all of the procedure. A health care provider monitors the patient throughout the procedure.
Conscious sedation is usually safe and effective in minimizing discomfort and anxiety during a medical procedure, and the medication wears off quickly after the procedure.
In the April 2016 issue of Physical Medicine and Rehabilitation Journal, four physicians shared differing opinions about the use of intravenous conscious sedation during a routine epidural steroid injection (ESI) to the lower back. A patient’s case is presented here, followed by a debate as to the best treatment plan. Drs Neel Mehta and Jennifer Zocca argue that conscious sedation should be offered to this patient. Drs Naum Shaparin and Max Snyder argue against the use of conscious sedation.
Patient case
Tom is a healthy 43-year-old man. Has been experiencing pain in his right leg for the last month; he has no other health issues. His pain starts in his right lower back and travels into the right thigh and calf. This type of back pain, which radiates to the leg is commonly referred to as sciatica.
After seeing his physician, Tom tries taking oral anti-inflammatory medications and completes 10 sessions of physical therapy without significant relief. During Tom’s physical examination, he experiences pain when he raises his straight right leg. Tom’s strength has not been negatively affected, and his reflexes are normal. A magnetic resonance imaging (MRI) indicates a herniated disk at the L3-L4 level that is pressing on the right L4 nerve root of his spine.
Tom’s physician offers a transforaminal lumbar epidural steroid injection (TFESI) as one strategy to potentially help alleviate his lower-back pain. On the day of the procedure, Tom’s pain score is 4 out of 10 at rest. His friend also received a TFESI with conscious sedation, and he requests the same.
Neel Mehta, MD, and Jennifer Zocca, MD, respond
Medical professionals have widely differing opinions and approaches to conscious sedation for interventional pain management procedures. A survey of 61 pain management centers found that 64% of pain management center used some type of sedation. However, for lumbar ESIs, fewer than half utilized sedation.
Benefits of conscious sedation
The primary goal of sedating a patient during an interventional pain management procedure is to reduce their anxiety and improve their tolerance of the procedure. This, in turn, helps the healthcare provider perform the procedure more easily.
Multiple arguments can be made for the careful use of sedation for interventional pain management procedures, which we will address in greater detail.
- Patients with chronic pain conditions are more anxious in general and, therefore, may be at higher risk for anxiety during the procedure than the general population.
- Some complications relating to anxiety, namely vasovagal reactions (a complex neurovascular reaction that occurs when the body overreacts to certain triggers) and hypertension, may be prevented with anti-anxiety medications.
- Certain patients prefer sedation for interventional pain procedures, especially when the option is discussed in detail before the procedure.
- It is possible that the use of conscious sedation to reduce anxiety and negative expectations may reduce the amount of pain experienced during the procedure.
Patients who have chronic pain—such as Tom—are, in general, more anxious than patients without chronic pain conditions. Persons with chronic neck or back pain are at a higher risk for panic disorder, agoraphobia, or social anxiety disorder and are almost 3 times more likely to have generalized anxiety disorder.
It is reasonable to expect that patients who are at higher risk for anxiety disorders, in general, are more likely to experience anxiety during a pain management procedure.
Complications related to procedural anxiety
Complications with interventional pain management procedures may be related to anxiety during the procedure. A vasovagal reaction is the most frequent adverse event reported from interventional pain management procedures. Stress, anxiety, fear, or pain associated with needles are the most common triggers.
One study attempted to identify patients at highest risk for vasovagal reactions with interventional pain management procedures and found that high-risk patients are twice as likely to be male, 2.4 times more likely to be younger than 65 years, and have lower pain scores before the procedure. It found that 30% of patients who had a vasovagal reaction required early termination of the procedure.
According to these statistics, Tom is at a higher risk for a vasovagal reaction.
Another consideration is the hypothesis that patient expectations, particularly negative expectations, may significantly influence the perception of pain intensity. Patients who have more anxiety and negative expectations surrounding a procedure often find the procedure to be less tolerable.
Physicians should evaluate patient anxiety, knowing that a highly anxious patient might be more at risk of a panic attack, resulting in unpredictable movement during critical portions of the procedure.
Patient preference
We believe it is reasonable, and even advisable, to discuss sedation with patients, particularly because many desire this option. Patients being treated with injections may have acute and chronic pain. Thus, they may find it challenging to be in the ideal position for the duration of the procedure.
When sedation was not discussed before the procedure, it was found that only 17% of patients requested sedation initially. When patients were surveyed after the procedure, however, this percentage jumped to 28% of patients who stated that they would ask for sedation for a subsequent procedure. These patients were found to have statistically higher reports of pain during the initial procedure. Moreover, when options for sedation were discussed in detail with patients before the procedure, 58% elected to have sedation when given a choice, and this number increased after the first intervention.
In general, interventional pain management procedures, including lumbar ESIs, are relatively safe. Several studies have compared patients given minimal to moderate sedation with those given no sedation and found no statistically significant difference in adverse events between groups.
The risks of conscious sedation can be mitigated, and patient safety can be optimized when health care providers with training in anesthesia and advanced cardiac life support certification administer the medicines.
In conclusion, using conscious sedation can be a safe and effective way to improve patient comfort and satisfaction, as well as minimize anxiety during pain procedures. For patients with significant anxiety or pain, sedation should be considered for even relatively short, uncomplicated procedures.
We believe conscious sedation will be beneficial for Tom.
Naum Shaparin, MD, and Max Snyder, MD respond
In 2010, the American Society of Anesthesiologists (ASA) Committee on Pain Medicine stated, “It is the opinion of the Committee that the majority of minor pain procedures, under most routine circumstances, do not require anesthesia care other than local anesthesia”.
Despite this recommendation, more and more patients who visit pain physicians expect to be sedated during routine procedures and often request sedation without prompting. We believe that physicians should not accommodate patient requests for unnecessary or unsafe treatments. We believe that conscious sedation is not necessary for Tom.
Most pain procedures, including lumbar ESIs, involve minimal patient discomfort and can easily be carried out with the use of a local anesthetic alone. Conscious sedation should only be considered in certain situations—such as the presence of other medical conditions, issues that inhibit adequate relaxation, or prolonged and excessively painful procedures—and when the benefits significantly outweigh the potential risks.
Risks of conscious sedation
What are the dangers associated with conscious sedation? It can make it more difficult for patients and healthcare providers to recognize important early warning signs of both neurologic injury and drug toxicity. A fully awake patient will be better able than a sedated patient to report pain or discomfort from needle contact with a nerve before potentially irreversible neurologic injury occurs.
The common medications used for conscious sedation cause breathing to slow to a certain degree, and there is always a risk that breathing can stop. An unrecognized decrease in breathing may lead to a drop in oxygen levels, which, if severe, can result in cardiac arrest. Most pain procedures are performed with the patient lying down, which makes accessing the airway challenging should an emergency arise.
Sedation during pain procedures is frequently given without a dedicated nurse anesthetist or anesthesiologist present for monitoring. Often, a registered nurse monitors the patient and administers sedating medications under the direction of the physician performing the procedure. Changes in breathing may be overlooked for an extended period while the physician is preoccupied with the pain procedure.
Finally, we are concerned that procedural sedation may affect the results of the procedure. The muscle relaxing properties of medications commonly used for sedation may cause the patient to believe that the procedure was more beneficial than it was.
Patients receiving sedation during their procedures may take extra time to rest after the procedure compared with those who did not receive sedation. The extra rest alone may improve the patient’s pain.
The costs of pain and sedation
Undoubtedly, pain is a significant problem in the United States. Pain treatment accounts for more than $100 billion annually between health care expenditures and lost productivity. Ensuring that patients have access to effective pain treatment is essential to ensuring that they recover fully and can return to the workforce.
However, utilizing sedation during pain procedures increases cost because of added medication, facility charges related to the provision of adequate recovery areas, and extended nursing/physician care costs during and after the procedure. The use of sedation also leads to logistical considerations, such as the need for an escort. No escort is required when performing procedures without sedation.
Our practice’s approach to conscious sedation
We choose to avoid sedation for routine pain procedures in our practice because offering or discussing sedation may lead to undue anxiety about the procedure that often overshadows the reality of the procedure itself.
Patients with chronic pain conditions, who also have anxiety disorders, can experience extreme worry and fear. This anxiety may contribute to worse outcomes in patients by allowing the pain to overwhelm their lives.
If a patient has anxiety, there are many lower-risk options than conscious sedation. Cognitive behavioral techniques aimed at teaching adaptive pain-coping mechanisms, such as hypnosis, biofeedback, and relaxation techniques, have become a core component of many multidisciplinary pain treatment programs.
Additionally, other simple techniques such as listening to music either before or during procedures have been shown to reduce patient anxiety level with no potential adverse effects.
The way patients approach their pain has a profound influence on their experience of that pain, as well as their emotional wellbeing. Simply taking the time to listen to the patient’s concerns and educating the patient about what to expect may be more useful than medications in alleviating concerns and anxiety. Most patients prefer additional information so they can prepare themselves and visualize the upcoming events.
In summary, offering sedation to all patients for routine pain procedures seems to significantly increase the possibility of adverse events or agitation, preventing a successful procedure. Conscious sedation has little, if any, guaranteed benefit.
For Tom, along with most of our patients, we suggest avoiding sedation and focusing, instead, on positive coping mechanisms.
Read more about pain-coping mechanisms.
Keywords
Fluoroscope: While an X-ray takes a single picture, a fluoroscope is like a continuous X-ray, providing real-time moving images that are used to guide the health care specialist during a pain management procedure.
Interlaminar ESI: An ESI to the back of the spine in the space between two vertebrae, which delivers the steroid over a wider area.
Interventional pain management: The use of techniques, such as injections or electrical stimulation, to directly address the source of pain.
Lumbar: Relating to the lower part of the back.
Transforaminal ESI: An ESI delivered into the opening at the side of the spine where a nerve root exits the spinal cord, allowing for more concentrated delivery to a particular nerve. (TFESIs are also referred to ask “nerve blocks.”)
Ultrasound: A diagnostic tool that uses sound waves instead of radiation. Like an MRI, an ultrasound gives provides a view of the soft tissue.
Vasovagal reaction or syncope: A reaction that occurs when your body overreacts to certain triggers, such as the sight of blood or extreme emotional distress. Vasovagal syncope causes your heart rate and blood pressure to drop suddenly, which leads to reduced blood flow to your brain and loss of consciousness.
References
A complete list of references supporting this article can be found in the original journal article.